Independent Orthopaedic Surgeons

Mr David Mitchell
MBBS (Melb), FRACS(Orth), FAOrthA, GAICD
- Knee Surgery
- Knee Reconstruction
- Patellofemoral
- Stabilisation
- Hip Replacement
- Day Surgery

Mr Luke Spencer
MBBS (Melb), FRACS(Orth)
- Shoulder Surgeries
- Hip Surgeries
- Knee Surgeries
- Re-alignment Surgery
- Reconstructions
- Stabilisation Surgeries

Mr Shaun English
MBBS, FRACS (Orth)
- Knee Surgeries
- Knee Replacements
- Arthritis Surgeries
- Hip Surgeries
- Hip Replacement
- Ankle Surgeries

Mr Scott Mason
BMedSci (Hons), MBBS (Hons), FRACS (Orth)
-
Knee replacement
and Arthroscopy - Hip Replacement
- Hand and Wrist Surgery
-
Shoulder and
Elbow Surgery - Foot and Ankle
- Trauma and Fractures

Mr Naveen Nara
MBBS, FRACS (Orth)
- Bunion Surgery
- Foot & Ankle Surgery
- Hip Replacements
- Knee Replacements
- Upper & Lower Limbs
- Trauma and Fractures

Mr Lawrence Tee
FRACS, FAOrthA
- Adult Spine Deformity
- Degenerative Spinal conditions
- Disc Herniation
- Hip Replacement
- Knee Replacement
- Trauma and Fractures

Mr Danie de Villiers
MBBS BMedSci FRACS FAorthA
- Shoulder Surgeries
- Hip Replacement
- Knee Replacements
- Upper Limbs
- Trauma and Fractures
- Arthritis Surgeries
Information
Anterior Cruciate Ligament Reconstruction
Cruciate reconstruction is an operation performed to restore stability of the knee. The majority achieve this, and a return to sport is the norm especially where no other injury has occurred to the knee.
The majority of cruciate reconstructions are undertaken with the patient’s own hamstring tendons. Other grafts might also have a place such as quadriceps tendon, patella tendon, or even an allograft transplant from a donor. A variety of ways to secure the graft to the femur and tibia are possible, such as Endobutton or interference screws.
The rehabilitation program is supervised by a physiotherapist – the usual scenario is 9-12 months, but special circumstances occasionally apply.
Are there syndesmotic injuries that can be treated non operatively?
The ankle syndesmosis refers to how the tibia and fibula are held together at the ankle joint. Because of the shape of the joint, the two bone should “spring” apart when weight placed through the leg. They don’t because the tibia & fibula are tightly bound together by the anterior and posterior inferior tibiofibular ligaments (AITFL, PITFL). When injured, the ankle is swollen and bruised, higher up than normal ankle sprains.
Severe injuries are universally treated surgically. Any fractures fixed, and then either one or two screws, or a suture construct between the two bone. If there is no fracture, usually the medial ankle ligament is torn. There is no clear superior technique, but untreated, 100% of the body weight goes through the top of the talus, where as normally, 40% of the weight is transmitted through the malleoli. Where screw fixation is used, it is often left in place three months, but walking permitted before the screw is removed.
A small proportion of cases, especially in athletes are isolated injuries to the AITFL. MRI might show the diagnosis but not prove whether any instability will occur. (Sensitivity for AITFL rupture 100%, specificity 93%, accuracy 96% (Takao JBJS Br 2003) In some patients then, the ankle will be stressed either with or without anaesthesia, either on x-ray testing or arthroscopy to fully assess. If stable, they are treated initially with a cast, RICE (Rest, Ice, Compression, Elevation) and then physiotherapy. They take typically three times longer to heal than a normal ankle sprain, ie three months might be needed.



Biceps Rupture
The biceps muscle in the upper arm has a tendon at either end. In the shoulder, proximal biceps rupture is very common, and might be only a minor part of other shoulder pathology. At the elbow, rupture of the distal biceps tendon is rare, but disabling. A bit like Achilles rupture, it occurs suddenly, due to a forceful activity, then more weakness than pain. Swelling and bruising ensure.
The vast majority should have surgery to restore the arm to full strength, it is easiest to operate early. Cases having surgery more than three weeks after injury are regarded as late. The surgery requires finding the tendon, and repairing to bone it through a bone trough in the radial tubercle.
Most commonly an Endobutton or Ziploop is pulled through the bone to maintain the tendon in position, much like is commonly done reconstructing the cruciate ligament in the knee. Partial rupture of the biceps tendon at the elbow is exceedingly rare, does need urgent surgery, but most likely pain will persist until a complete rupture occurs.

Tennis Elbow
Tennis Elbow can be a debilitating condition causing pain over the outer aspect of the elbow. It seems to be caused by tiny tears in muscle and tendon fibres and is common in middle age.
There are similar conditions with Golfers Elbow on the inner aspect of the elbow, and some types of Achilles tendonitis.
Non operative treatments include physiotherapy, stretching exercises, eccentric training, and sometimes activity modification. Surgery is only rarely indicated, leaving a large number of people who are frustrated!
Cortisone injections for tennis elbow work temporarily, in 50% people they seem to be curative.
The current trend is toward treating these conditions with Autologous Blood Injections (ABI). Some of your own blood is mixed with local anaesthetic, and injected into the damage tissue.
This seems to incite a healing response, doctors often talk about the growth factors in the injections, and some surmise there are more growth factors in part of the blood, platelets.
For the appropriate cases, I do Autologous Blood Injections (ABI).
This is a simple procedure performed in the rooms taking 15-20minutes, and has substantially reduced the number of these cases needing surgery in my hands.
Golfer's Elbow
Golfer’s Elbow can be a debilitating condition causing pain over the inner aspect of the elbow. It seems to be caused by tiny tears in muscle and tendon fibres and is common in middle age.
There are similar conditions with Tennis Elbow on the outer aspect of the elbow, and some types of Achilles tendonitis.
Non operative treatments include physiotherapy, stretching exercises, eccentric training, and sometimes activity modification. Surgery is only rarely indicated, leaving a large number of people who are frustrated!
Cortisone injections for golfer’s elbow work temporarily, in 50% people they seem to be curative.
The current trend is toward treating these conditions is Autologous Blood Injections (ABI) . Some of your own blood is mixed with local anaesthetic, and injected into the damage tissue.
This seems to incite a healing response, doctors often talk about the growth factors in the injections, and some surmise there are more growth factors in part of the blood, platelets.
For the appropriate cases, I do Autologous Blood Injections (ABI).
This is a simple procedure performed in the rooms taking 15-20minutes, and has substantially reduced the number of these cases needing surgery in my hands.
Clavicle Fractures
Clavicle fractures had quite a discussion at the 2015 Australian Orthopaedic Association Annual General Meeting in Brisbane. The results of surgery perhaps are not as good as we’d like – whether it be fixed with screws or plates. The results of a non surgical approach probably are fine in 90% of cases, but perhaps 10% ultimately come to surgery for non union, or non-union, of the fracture.
After surgery, a sling is required for a short period of time, and then gradually return to function. Risks of this surgery can not be understimated, even deaths have been reported in the world literature for fixing clavicles. Time to return to sport depend on the nature of the fracture and whether plate or screw used.

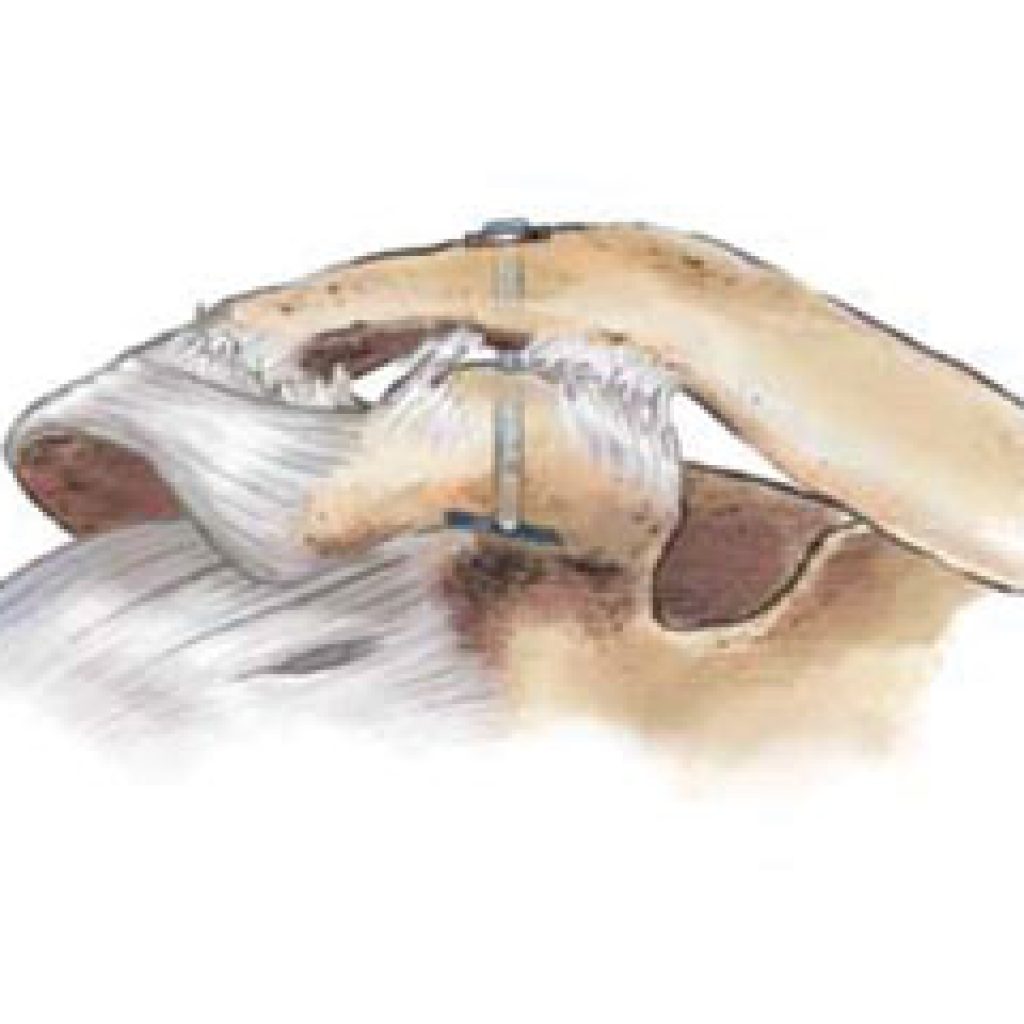
Shoulder ACJ dislocation & injury
Acromioclavicular joint (ACJ) injuries are common. The minor sprains are treated with analgesics, anti-inflammatories, physiotherapy and rest. The more severe types need surgery. The most common type is grade 3, which becomes less prominent when the shoulders are shrugged where as type 4 & 5 get worse when shoulders are shrugged. The treatment of type 3 is controversial – surgery means more time in a sling, and the result possibly no better at one year.
Classification of ACJ injuries (Rockwood 1998)
Sprain of AC ligaments
- Rupture of AC ligaments and partial rupture CA (coracoacromial) ligament
- Complete rupture of AC & CA ligament, 100% displacement.
- AC & CA ligaments and deltotrapezial fascia perforated by clavicle backwards
- AC & CA ligaments and deltotrapezial fascia perforated by clavicle upwards (>25mm)
- Rare – ligaments ruptured and clavicle under corocoid!



Shoulder calcific tendonitis
Acute calcification of the shoulder is very painful. Some people require strong narcotic medications for the pain in addition to simple analgesics like paracetamol and anti-inflammatories. It might spontaneously resolve, but not always. If the pain is severe or persistent, surgery is often recommended.
The attached video demonstrates the calcium being squeezed out of the rotator cuff. This “pimple” of calcium and the angry tissue around it gets squeezed every time the shoulder is moved up, so its hardly surprising patients come asking for it to be fixed!
Chronic calcification is similar, but more difficult to get out, and might require tendon repair surgery at the same time. Sufficient people settle without surgery for us to know that surgery isn’t required for everyone. But “if pain persists…..”
Hip Injuries – Hamstring Tears
“Doing a Hammy” is not always the same injury. Most commonly, it is a partial tear within the muscle, and anti-inflammatories and physiotherapy are all that is required (and of course more stretching before exercise next time!). If it’s sore to touch in the buttock, perhaps it’s a tear off the pelvis, but still usually it’s a partial tear, and reasonable to treat the same. If a partial tear doesn’t settle, it can easily be treated later.
Complete tears of the pelvis is rare, but we see it particularly in water skiers, footballers, and a variety of other injuries. The bruising is usually dramatic, extending well down the thigh. The problems we see in this group are persistent weakness, pain running, and an inability to return to sport. And the surgery to fix it is more difficult if performed late, as the hamstring becomes severely scarred to the adjacent sciatic nerve. For this reason this group tends to have surgery early.
It is possible to operate late on incomplete tears relatively easily. Late repairs of complete tears are difficult. The adjacent nerve needs to be dissected free, the tendon brought back up to the pelvis and stitched into place.The further pulled away, the surgery is more complex, the incision longer, the nerve risk higher, and the recovery more difficult.
The patient has greater risk, and a more difficult recovery, sometimes requiring the foot to be hitched to the back of a belt for some weeks. To avoid these problems, we have more athletes having surgery early after complete hamstring tears.

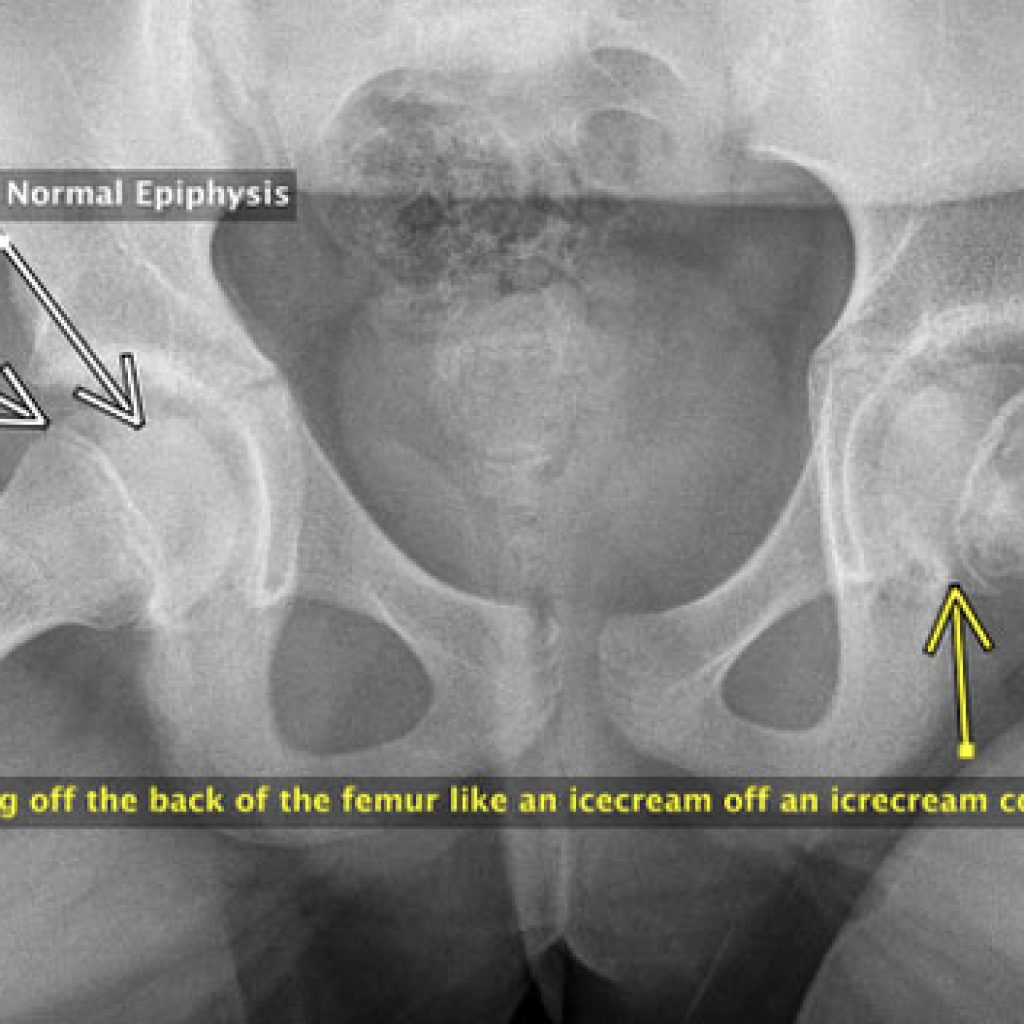
Slipped Femoral Epiphysis
Slipped epiphysis (SUFE, SCFE) is a relatively uncommon childhood condition where the ball of the femur in the hip joint slides off the back of the femur to a small or large extent. The problem occurs in the growth plate of the hip (physis) the head part is the epi-physis.
It causes pain in the leg – it can be over the knee, but might be in the thigh or groin. If the slip is severe, the leg points outwards. If acute, the pain can be severe and the child unable to walk. If more subtle and subacute, the limp might be the most obvious feature.
If the initial concern is the knee, and health practitioner finds nothing wrong with the knee, then x-ray of both hips is required to be sure the cause of the problem isn’t a slipped epiphysis.
Our practice has done the majority of cases in Ballarat and district over the last decade – either at St John’s or through Ballarat Base Hospital. Some severe cases are transferred to Royal Children’s Hospital for consideration of correcting the deformity rather than simply fixing it in position.

Adolescent injuries around the hip
From the Journal of Paediatric Orthopaedics is a review of 228 apophyseal avulsions of the pelvis. 49% were from the anterior inferior iliac crest (AIIS), 30% ASIS, 11% ischial tuberosity, 10% iliac crest. The majority (97%) were treated non operatively.
The most troublesome group was the AIIS with ongoing pain. Failing to heal was most seen with fragments more than 20mm displaced and/or of the ischium.
They concluded that most cases are treated without surgery, and the reasons to operate are displaced AIIS fragments or gross displacement.

Meniscal Repair
Arthroscopic meniscal repairs have been reported since 1986. Some meniscal tears are still better treated with an additional open incision – the lateral meniscus posterior to the popliteal hiatus is perhaps the best example.
Successful results require any instability to be addressed, a well aligned knee and augments to meniscal repair such as fibrin clot, vascular access channels, and synovial abrasion are routine. Most common tears repaired are peripheral tears, bucket handle tears, but it is also possible to repair some horizontal cleavage tears.
More recently, meniscal root tears have been identified as tears that cause a rapidly progressing arthritis as the mensicus is often “extruded” from the joint, functioning as a total mensiectomy.
These too can be repaired into a prepared bone tunnel with transtibial sutures although other techniques are being developed.
Meniscal Transplant
Meniscal allograft transplantation (MAT) is a valid consideration in patients with post menisectomy pain, in a well aligned, non arthritic knee. Luke Spencer has fellowship training in MAT and has undertaken a number of cases since joining our group.
Patients who are mal-aligned need corrective osteotomy in addition to the MAT.
Patella Dislocation

There are many reasons why children and young adults can have a kneecap dislocate.
Probably half of them are because of trauma alone, the others might have lax ligaments, a flattened grove the kneecap tracks along, in-toeing gait, long patella tendon, knock knees, or any combination.
These are not easy cases to sort out. Typically with a first time dislocation, an arthroscopy & washout might be undertaken to speed up the recovery process especially if the knee is still very swollen and loose fragments are suspected.
Physiotherapy and taping are then usually instituted. If there is a significant concern the dislocation might become recurring, corrective surgery might be undertaken.

1. MPFL reconstruction
The most common operation is to reconstruct the damaged ligament from the inner aspect of the femur to the kneecap.
In this case, drill holes through the kneecap hold the hamstring graft at one end, the screw in the femur holds the graft in a tunnel.
Some surgeons use screws that cannot be seen on x-ray, either way, the screw is usually left permanently.
2. Faulkerson Procedure.
This operation can be applied to many cases including cases where the patella tendon doesn’t line up well, those with kneecap pain, patients with a combination of problems even ligamentous laxity.
In this operation, the boney prominence that the patella tendon connects to the tibia through is surgically moved and screwed into its new position, some soft tissue surgery is also undertaken.
3. 8-Plate Correction of Knock Knees
This operation using “8-plates” is performed to gradually correct knock knees, in doing so the direction of pull of the patella tendon is corrected.
Some might still need a ligament reconstruction, but this surgery on growth plates is quite time critical, before the growth plates close. The typical girl would need this by 13 years of age, and perhaps 15 for boys.
The surgery is done through a 1cm cut for each of the four plates, sometimes only one leg, or only one growth plate per knee needs to be corrected.
4. Other operations
Other operations include deepening the groove the patella tracks in, rotating the femur either near the hip or knee joint.
In some acute cases, it might be possible to repair the damaged MPFL (ligament) but often much of the ligament has been stretched as well as the obvious injury.
Multi Ligament Knee Injury
The knee ligaments allow the smooth cartilage surfaces of the knee to remain stable during range of motion, impact, and pivoting/twisting activities. Ligaments are the tissues that join one bone to another. Tendons join muscles to the bone. The knee has multiple ligaments and tendons.
The major ones include the: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), fibula collateral ligament (FCL), postero-lateral corner (PLC), anterolateral Ligament (ALL) and posterior oblique ligament (POL). The postero-lateral corner includes the FCL, Popliteo-fibular ligament and Popliteus tendon.
High-energy knee injuries can lead to devastating consequences for stability, from injuries to more than one of the critical knee stabilisers. Multi-ligament knee injuries are very serious.
With severe injury the entire knee can even dislocate and lead to tearing and damage to the nerves and even blood vessels. This can cause critical damage to the blood supply of the leg requiring vascular operations or potentially amputations.
Ankle Sprain
We don’t routinely use ultrasound to assess ankle injuries.
A plain x-ray excludes ankle fractures & 5th metatarsal base fractures.
If the bruising is typical of a sprain, and x-ray is normal, physiotherapy is appropriate.
For normal sprains, early physiotherapy is the most appropriate treatment. If not behaving as expected, orthopaedic assessment is reasonable.
ATFL injuries alone do not require orthopaedic care, 95% will heal with conservative management, and few require reconstruction for instability.
Indications for surgery after normal ankle sprain are ongoing pain or ongoing symptomatic instability.
Red flags are:
- excessive swelling that extends above the ankle suggests a syndesmosis sprain.
- excessive swelling below the ankle on both sides sometimes represents a subtalar joint injury.
- an inability to weight bear is unusual for an ordinary ankle sprain by a day.
Plantar Fasciitis
Not all heel pains are caused by plantar fasciitis. It refers to a very specific, localised pain under the heel, in the absence of other pathology.
Non operative treatment can be soft heel inserts, or an orthotic with a cutout under the painful area, and anti-inflammatory tablets. Stretching exercises may help.
Injections have reasonable results – up to three injections of cortisone are possible. Some sports medicine doctors are now using blood or PRP injections.
The pain seems to be caused by the recurrent micro tearing, the bone spur is the result, but rarely important in the pain.
Shock wave treatment has become our main treatment, and involves a number of visits to our sports medicine department. The results seem virtually the same as the surgical success rate.
Surgical treatment is occasionally undertaken, endoscopic release of 80% of the plantar fascia, but carries its own risks. Patients with the most successful surgical outcomes are thin, athletic, not diabetic and have only one foot involved.
Osteochondritis Dessicans (OCD) of the knee
During development, cartilage is slowly replaced by bone. This leaves a thin shell of smooth joint surface lining cartilage that covers the underlying bone. Occasionally, a piece of the underlying bone separates with the overlying cartilage remaining intact (stable OCD lesion).
However, when the overlying cartilage separate with the bone, joint fluid can wash under the bone and prevent bone healing (unstable OCD lesion). In severe cases the bone and cartilage fragment can become loose within the joint. The most common joint involved is the knee, but also the ankle and elbow can be affected.
This process occurs during development, usually around the ages of 10 to 15.
The younger the onset, the more likely the lesion will heal on its own, with restriction of activities and sports for a period of 6 months or more. A larger lesion presenting at a later age is less likely to heal on its own.
Sport Injury Treatments & Surgeries Available
- Biceps Rupture
- Tennis Elbow
- Golfer’s Elbow
- Clavicle Fracture
- Shoulder Dislocation
- Shoulder ACJ dislocation & injury
- Shoulder calcific tendonitis
- Shoulder Tendon Injury
- Hip Injuries
- Hamstring Tear
- Hip dislocation
- Slipped femoral epiphysis
- Adolescent injuries around the hip
- Hip pain from dysplasia
- Knee Injuries
- Biological Knee Reconstruction
- Meniscal Repair
- Meniscal Transplant
- Cartilage Grafting
- Patella Dislocation
- ACL (Anterior Cruciate Ligament) Injury
- Multi Ligament Knee Injury
- Achilles Rupture
- Achilles Tendonitis
- Ankle Sprains
- Ankle Ligament Reconstruction
- Ankle Syndesmosis Injury
- Ankle Arthroscopy
- Plantar Fasciitis
- Treatment of OCD (Osteochronditis Dissecans) lesions in knee and ankle
- Lumbar discectomy
- Spinal decompression
- Spinal fusion
- Interbody fusion
- Cervical spine surgery