Knee Arthroscopy
Knee Arthroscopic Meniscectomy
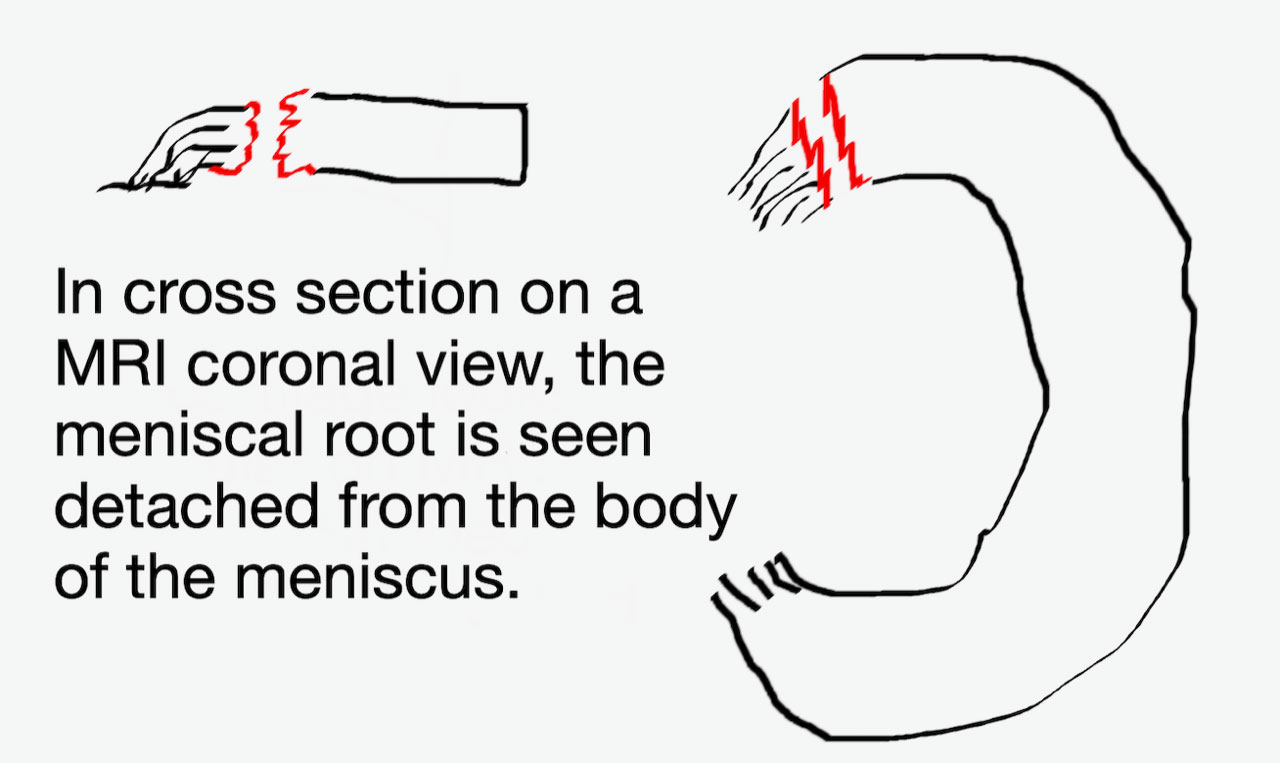
Knee Arthroscopic Meniscal Repair
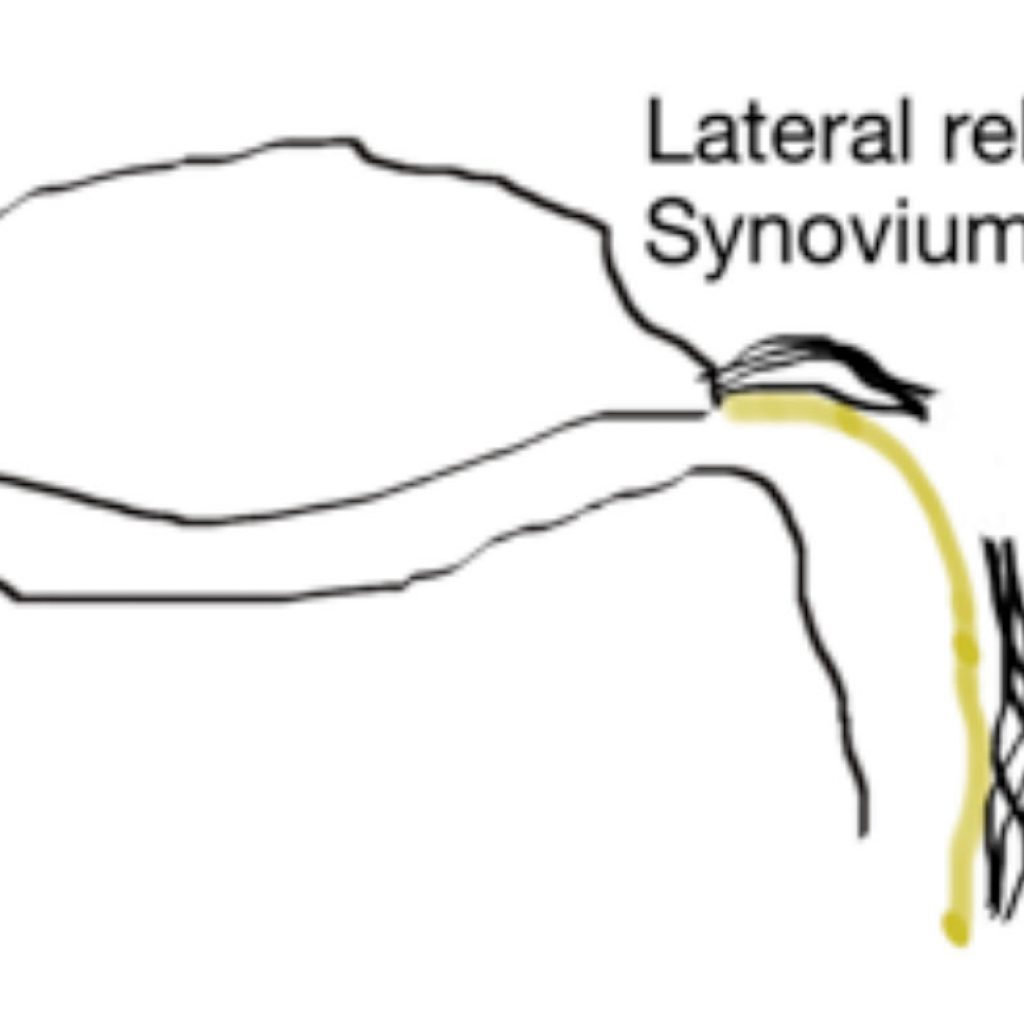
Knee Arthroscopy & Lateral Release
Knee Arthroscopy & Arthritis
Knee Replacement Surgery
Anterior Cruciate (ACL) Reconstruction
Multi-ligament knee injuries
Patellofemoral instability surgery
Osteochondritis Dessicans (OCD) of the knee
Knee Realignment Surgery
Meniscal Transplants
Cartilage (Chondral) Defects
Patella Pain Surgery
- All
- Sports Medicine
- Orthopaedics
- Novar Specialists

Sports Medicine

Hands and Wrists

Knees

Rapid Recovery Surgery

Psychology

Shoulders & Arms

Physiotherapy

Medical Clearance Assessments

Joint Replacement

Foot & Ankle

Hips & Hamstrings

Trauma

Spine Surgery

LIPUS

Shockwave Therapy

Neurology

Myotherapy

Exercise Physiology

Tendon Treatments

PRP Injections

Iontophoresis

Autologous Blood Injections (ABI)
