It has been long known that the meniscus is a key structure in the knee providing load share for the joint surface.
In the knee joint, the tibial surface is flat, the femoral surface convex, the meniscus is a convenient pliable structure that allows conformity between these two surfaces and even load transmission. Without it, the contact forces are doubled or more. With the meniscus, the compressive forces are converted to “hoop stresses” pulling on the meniscal roots, avoiding extrusion of the meniscus.
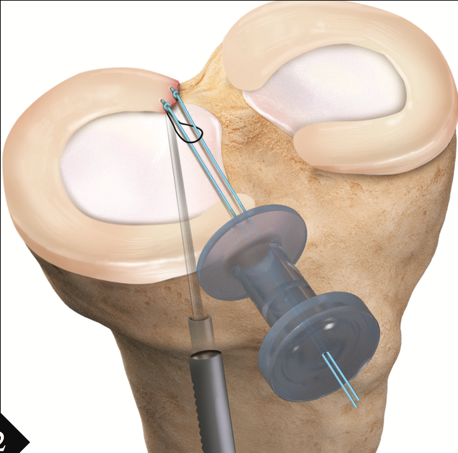
Meniscal root tears have been discussed extensively in the arthroscopic journals since 2014, where they occur within 5-10mm of the posterior tibial insertions, the meniscus can be mobilised and repaired to bone. Often the medial collateral ligament needs a partial release to achieve exposure, and this heals well. The bone tunnels drilled for the sutures allow bone marrow stems cells to bath the region of repair. Because of the forces involved, the patient is required to use crutches typically for three months. Overweight patients and middle aged patients have as much to gain through these repairs as anyone – and surprisingly the results are just as good in these groups.
Horizontal cleavage tears also have had improvements in their treatment. Although they are usually regarded as “degenerate” they typically extend to the periphery of the meniscus, thus have access to the “red” zone of the meniscus. Previously the less important leaf of the meniscus has been resected, but the same overloading of the articular cartilage occurs as in the meniscal root tears. Where a parrot bear tear or the like has occurred, there may not be a better treatment than resection, but if the patient has the patience for the curative treatment and time on crutches, it is the right thing to do. A surprising finding has been that having meniscal sutures over the “sharp” inner edge of the meniscus does not cause a problem – in time the sutures become incorporated into the meniscus, whilst the maximal number of circumferential collagen fibres sharing the hoop stresses are maintained.
Where practical, for the ideal horizontal cleavage repair:
the patient is under 40
synoviocytes are removed from the tear with shaver or rasp
a fibrin clot is interposed in the repair
if there is malalignment of the leg, a corrective osteotomy is performed
Where practice, for the ideal meniscal root repair:
the tear is near the meniscal root
arthritic changes are minimal (No worse than Outerbridge 2)
if there is malalignment of the leg, a corrective osteotomy is performed
LaPrade’s classification of meniscal root tears (2015)
1 – Partial, undisplaced tears
2A – Complete radial tears within 3mm of boney attachment
2B – Complete radial tears within 6mm of boney attachment
2C – Complete radial tears within 9mm of boney attachment
3 – Bucket handle tears with complete detachment of root
4 – Complex oblique tears with complete detatchment extending into root
5 – Boney avulsion fracture of root
Forkel & Peterson classification of lateral meniscal root tears (2012)
1 – Root avulsion with intact meniscofemoral ligament
2 – Radial tear of posterior horn with intact mensicofemoral ligament
3 – Complete rupture of posterior horn including meniscofemoral ligament
Mr David Mitchell
Orthopaedic Surgeon