Do you know the most common injuries in Water Polo?
The Victorian Country Water Polo Championships were held in Ballarat this year. Ballarat Water Polo one of the newest clubs in regional Victoria and is well represented by the local medical community with our BallaratOSM Practice Manager, Mr Adrian Warmington and Lake Imaging Radiologist, Dr Alex Meakin both executive members of the committee.
After a blow last year when Ballarat were unable to run the Championships due to a snap lockdown, this year forged ahead as planned. The tournament had 160 players, plus officials, and spectators supporting the event and local community.
Congratulations to Albury Sharks for winning the Women’s title, in a nail-biting penalty shoot-out with the Geelong Marlins. The Albury Tigers made it a double by taking the championship title for the Men’s competition.
Like any sport water polo can result in injury. Water polo players need to be able to move quickly, explosively and efficiently in order to avoid being pushed or hit, and to prepare for attack. You need to be in control of your shoulders, back, hips and knees – all at the same time.
Concussions and facial injuries are typical acute injuries among water polo players. These occur when the head is hit by an arm or the ball. The shoulder can also be injured when defense players try to block an attack. Muscular contusions from blows or pulled muscles also occur. Knee pain is also not uncommon. Because of the nature of the sport, many players are also susceptible to overuse injury that can cause prolonged problems in the knees, shoulders and low back.

- Concussion
- Facial injuries (teeth, eye, skin)
- Labrum tear (SLAP-lesion)
- Rotator cuff injury
- Patellofemoral pain syndrome
- Back pain
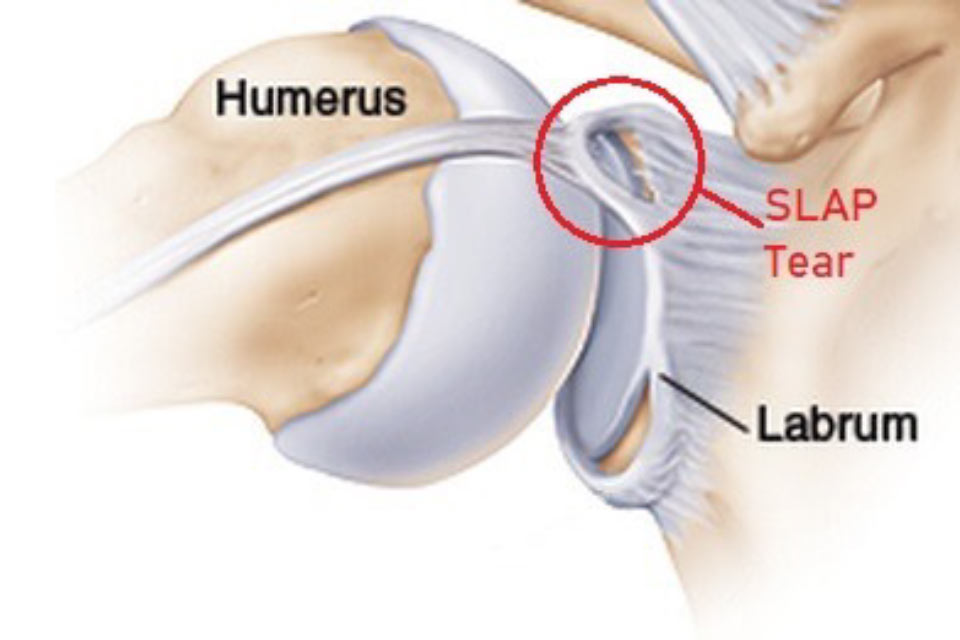
Labrum tear (SLAP-lesion)
The glenoid labrum is a cartilaginous rim that stabilizes and protects the shoulder joint. Labrum injuries often occur in throwing sports and sports where the arm is frequently raised above shoulder height.
The labrum is located where the upper arm attaches to the shoulder blade. It surrounds the head of the upper arm and thereby increases the stability of this joint during shoulder movements. The most common labrum injury is called a SLAP lesion. It occurs in the upper part of the cartilaginous rim, where the biceps tendon attaches.
The labrum can be damaged as a result of an acute injury and also as a result of an overuse injury from repeatedly performing a throwing movement with high forces. As such, SLAP lesions are common in throwing sports like water polo where the arm is frequently used above shoulder height.
A common symptom of a SLAP lesion is pain in the upper or back part of the shoulder. The shoulder can also feel unstable, and there might be a sensation of “catching” or “clicking” in the joint.
Treatment
The first step in treatment will always be a rehabilitation period of at least 3 to 6 months with guidance from a physiotherapist or Sport & Exercise Medicine physician. If there is no improvement during this time, surgery may be considered. The surgeon will often determine how much the injured person should be allowed to move their shoulder once the surgery is completed. It is important to follow these restrictions as it allows healing to take place.
Between 80 to 100% of athletes return to sport following surgery, but only 50 to 60% of these can perform at the same level as before.
Rehabilitation
In the first phase following surgery and until the injured area has fully healed, it should be kept immobile. This usually takes up to 6 weeks. During rehabilitation it is important to train:
- Mobility
- Interaction between the muscles
- Movement control
- Strength
Impingement of the rotator cuff
The rotator cuff is a term for the muscles around the shoulder blade. Shoulder impingement is a very common cause of shoulder pain in athletes, it is considered an overuse injury.
Shoulder overuse injuries in athletes often occur when they perform many repeated movements. The tendons of the muscles can also be injured if they become impinged between bones in the shoulder joint during certain movements, such as throwing.
Injury to rotator cuff tendons usually happens gradually. In the early stages, pain can actually be felt without the occurrence of any structural damage. In later stages the tendon tissue can become weaker. This is known as tendinosis, and it can ultimately result in the partial or complete rupture (tearing) of the tendon.
Tendinosis of the rotator cuff is very common among athletes in sports that involve a lot of movement with the arms raised above shoulder height such as water polo. This activity places extreme demands on the shoulder.
Impingement
Impingement is one of the most common causes of shoulder pain in the rotator cuff. It results from a tendon becoming pinched between the upper arm and the shoulder blade (scapula) in certain positions when the arm is raised.
There are two main types of impingement: subacromial impingement. This is when the arm is raised straight up above the head, and posterior impingement, which occurs when the arm is held all the way back in a throwing position.
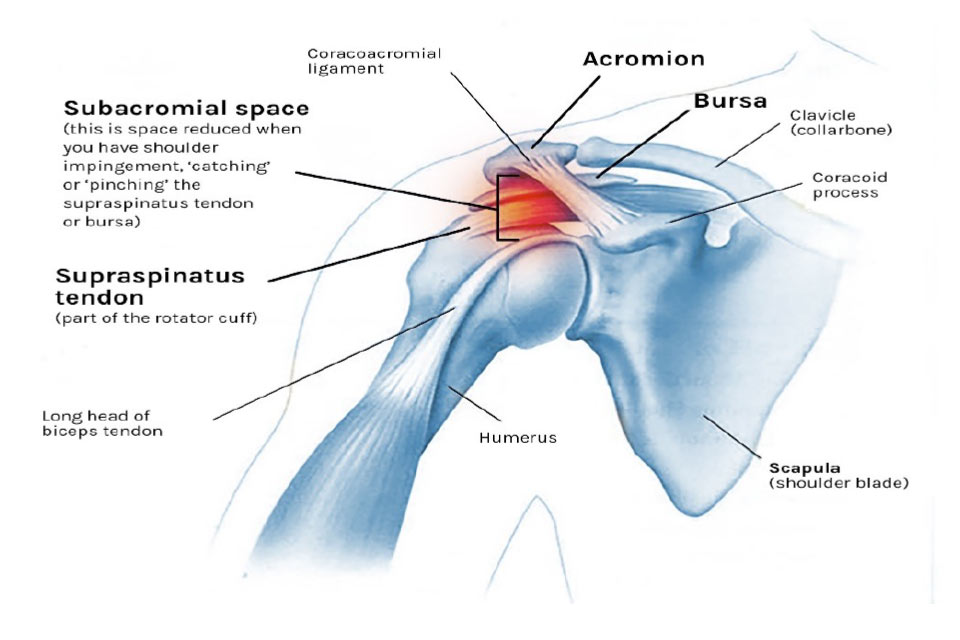
Subacromial impingement
Subacromial impingement occurs in the so-called subacromial space between the head of the upper arm and the top of the shoulder blade where they make up the shoulder joint. The supraspinatus tendon (one of the rotator cuff muscles) is most often affected. In addition, other structures such as a fat pad (subacromial bursa) can also be affected. Given that several structures can be involved, we often refer to this as impingement syndrome.
Subacromial impingement syndrome can be caused by variations in shoulder anatomy, muscle tightness, a stretched joint capsule or due to a lack of stability from the muscles around the shoulder blade. A common and effective way to treat this is to use an individualized training program. If conservative treatment fails, surgery can be performed to increase the subacromial space. Subacromial impingement is most common among people aged above 45, but it can also occur in younger athletes.
Posterior impingement
Posterior impingement is common amongst athletes in sports where the main activity is above shoulder height. The condition concerns the tendons of the infraspinatus and supraspinatus muscles and occurs when the shoulder is held all the way back in a throwing position. Typically, athletes with posterior impingement experience pain in the back of the shoulder when in this position.
Posterior impingement can be caused by a lack of control and stability of the shoulder blade when throwing. Poor throwing technique can be a contributing factor.
Treatment and rehabilitation
The first step in treatment for almost all injuries of the rotator cuff is an individualized rehabilitation program. During rehabilitation, the athlete should be removed from the activity or sport that caused the injury. A physiotherapist or Sport & Exercise Medicine physician should supervise the program and focus should be on specific factors such as:
- Mobility of the shoulder
- Strength and coordination of the rotator cuff
- Control of the shoulder blade
- Sport specific training (for example, in throwing sports strength and mobility of the hip, upper back, and shoulder are very crucial)
It is imperative that the load and demands on the shoulder are increased gradually so that the athlete can fully participate in the sport without experiencing pain. This approach is successful in the majority of cases, even when there is considerable structural damage to the tendon such as with a full thickness tear. It often takes up to 6 months of rehabilitation before any significant improvements are noticeable.
Sometimes a cortisone injection can be of help in relieving the pain and allowing rehabilitation to proceed. A cortisone injection usually will not fix impingement by itself, and is best done with ultrasound or some other form of imaging guidance.
If conservative treatment is unsuccessful, surgery should be considered. However, surgery should not be viewed as a quick-fix solution. Recent research shows that around 25% of athletes in throwing sports don’t return to sport following surgery to the rotator cuff, and only a small percentage of those who do return manage to do so at their pre-injury level of performance. Also, rehabilitation following surgery takes a long time. The average duration for a return to sport is 12 months.
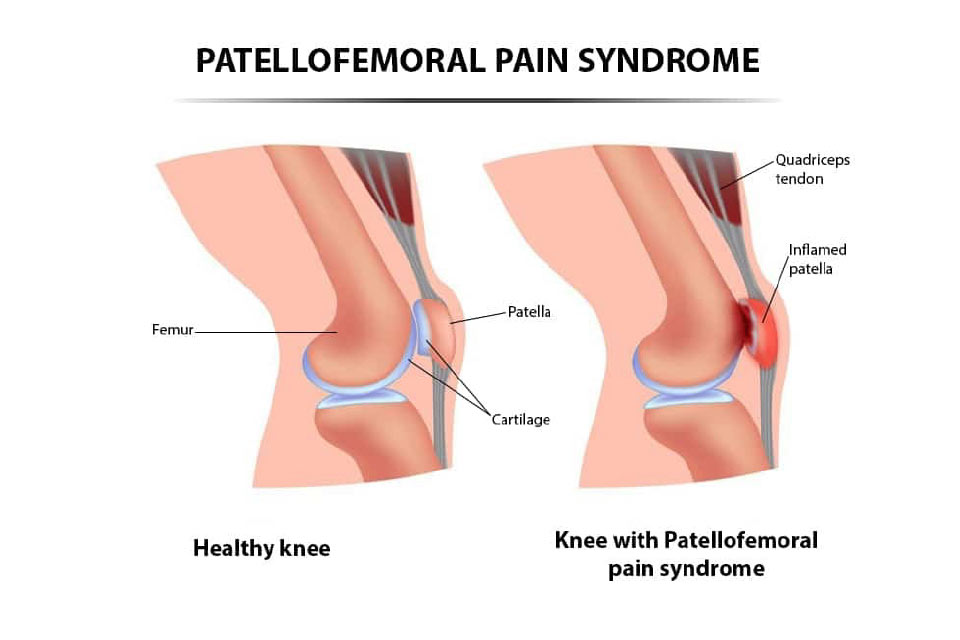
Patellofemoral pain syndrome
This condition is characterized by diffuse pain in and around the kneecap without a specific cause. Knee pain is extremely common in adolescents who play sports.
Studies have shown that around 50% of non-specific knee pain (pain of unknown cause) may be due to patellofemoral pain syndrome (PFPS). PFPS is common in running sports and cycling and most often seen in those between 16-25 years of age.
PFPS may be caused by several factors, and with athletes it can be related to excessive overload. PFPS can also be caused by direct trauma to the kneecap, for example by falling on it, even though this is much less common.
Symptoms
The most common symptom is a diffuse pain in and around the kneecap without having an injury. The pain is aggravated by using stairs (especially going down), squatting, cycling, and with prolonged sitting. It is uncommon for the knee to lock-up or give-way, as is common with other knee injuries and conditions. The knee may feel stiff, even though it still has normal flexibility. Noises from your knee are common and not a sign of damage.
Diagnosis
A doctor, Sport & Exercise Medicine physician or a physiotherapist will take your medical history and conduct a physical examination to confirm the diagnosis. X-ray and MRI images are often normal and are therefore of limited use.
Risk factors
We do not know exactly what causes PFPS. Some anatomical and biomechanical factors have been suggested as risk factors for developing the condition. Examples include overpronation (when the foot lands on outside of the heel and rolls inward), reduced strength and hip control. It is also likely that the training volume and intensity may play an important role. When anatomical factors are combined with overuse, there may be a risk of developing PFPS.
Gender is also considered a risk factor; female athletes have 1.5 – 3 times higher occurrence of PFPS than their male counterparts.
Treatment and rehabilitation
The treatment of PFPS requires a holistic approach that considers all the potential factors that might have caused the condition. For some it might be appropriate to focus on strength, mobility or muscle control. This is usually done with a structured training program. It is advised to consult a physiotherapist or Sport & Exercise physician who has expertise in dealing with this condition.
Load management
Load management is one of the most important aspects of effective treatment and the athlete’s total training load should be summarized and evaluated. It is often necessary to reduce the amount of pain provoking activities for a short period. Using orthotics (knee braces) and tape may reduce symptoms, but often temporarily. They can, therefore, be used as part of the overall treatment strategy. The return to sport should be gradual and well structured. Good communication and collaboration with the coach are recommended throughout the rehabilitation.
For more information about water polo injuries visit https://fittoplay.org/sports/water-polo/the-most-common-injuries-in-waterpolo/
The Ballarat Sports Medicine and BallaratOSM teams are always available to assess, diagnose and treat your injuries.
Contact us to see our Physiotherapist, Sport & Exercise Medicine physicians, Rehabilitation Physician and Orthopaedic Surgeons.
