Whilst severe pelvic fractures are treated by orthopaedic surgeons in trauma centres, spontaneous sacral insufficiency fractures might be treated by endocrinologists, or rehabilitation physicians. But here are my comments!
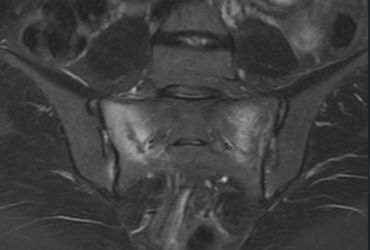
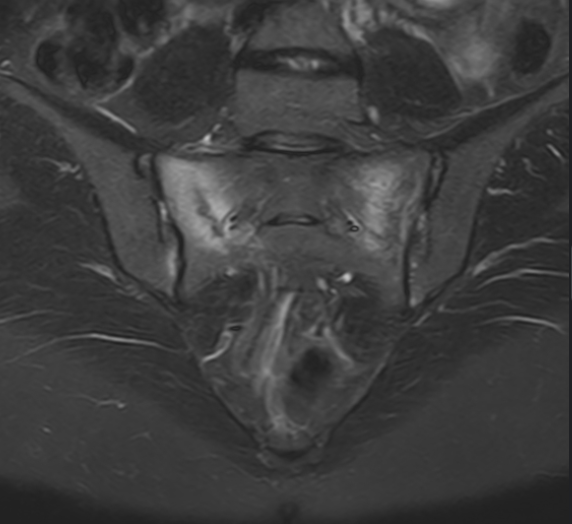
Typically the presentation is low back / pelvic pain, usually it can be localised to the junction of the pelvis and the spine, worsening with activity. Groin pain and even sciatica pain can occur. MRI diagnoses a crack, or cracks in the pelvis. It can occur in osteoporosis, vitamin D insufficiency, possibly over hormone imbalances, possibly also as an athletic overuse injury (where it is usually called a stress fracture). Screw fixation, and sacroplasty (injecting bone cement) are higher risk, and probably lower success than medical management.
Management includes:
- Activity modification check, and treat vitamin D deficiency – normal range is 50-200 nmol/L – at least be in middle of range!
calcium supplements analgesics – antiinflammatories – meloxicam (Mobic) 15mg daily, paracetamol – take strictly until the dust settles top up analgesics – tramadol (Tramal) or tapentadol (Palexia) are better than opioids.
Then it gets tricky. There are bisphosphonate medications that help osteoporosis have a role – but perhaps not until the fracture has healed? Alendronate is an example. Raloxifene is almost as good with less problems of osteonecrosis. Calcitonin seems less effective than recombinant human parathyroid hormone – teriparatide (Forteo). Teriparatide is an injection treatment that has been shown to reduce pain & disability better than “sacroplasty” by one month. It’s a daily injection for six months. Presumably prescribed by the rehabilitation or endocrine doctors. The alternative of sacroplasty is a radiology trick under CT control, injecting “bone cement” into the sacrum. But with Teriparatide doing better, it seems the better treatment – except if additional conditions – for example Paget’s disease of bone, or metastatic bone disease.
References:
- Yao-Chun Yang, Min-Hong Hsieh, Jui-Teng Chien, Keng-Chang Liu, Chang-Chen Yang, Teriparatide treatment shows faster healing than sacroplasty for postmenopausal women with sacral insufficiency fracture. Osteoporos Sarcopenia. 2023 Feb 15;9(1):27–31. doi: 10.1016/j.afos.2023.02.00
- Praise Briggs, Samuel W King, Tim Staniland, Shivkumar Gopal, Rajesh Shah, Mukai Chimutengwende-Gordon. A Systematic Review of Sacral Insufficiency Fractures: Treatment Modalities and Outcomes. Cureus. 2023 Jul 11;15(7):e41745. doi: 10.7759/cureus.41745
Blood tests to consider:
Levels of thyroid-stimulating hormone (TSH), parathyroid hormone (PTH), calcium, phosphorus, albumin, 25-hydroxyvitamine D, urinary calcium, creatinine, full blood count, liver function tests, C-reactive protein (CRP) and erythrocyte sedimentation rate (ERS) must be investigated if secondary osteoporosis is suspected. Serum levels of alkaline phosphatase (ALP), a marker of bone formation, are often slightly raised and this should lead clinicians to consider the differential diagnosis between stress fractures and an active form of Paget’s disease.
David Mitchell
Orthopaedic Surgeon