We have recently gained Federal Government recognition as a Specialist Training site, which means you can see our Sports Doctor, Dr James Ooi, for no more than $50 out-of-pocket for a standard appointment. Physiotherapy appointments can be partly claimed from your private Health Insurance extras. Any braces/crutches/other items will be charged separately.
How long is the appointment?
Our standard medical appointments are 40 minutes long for new problems.
How will this help you?
Early treatment of sporting and other injuries greatly improves both the speed of recovery and how well you recover. The reason that elite athletes can return to play within a few weeks of a serious injury is mainly due to them spending the first few days treating the injury properly. While this sounds simple, it is easily neglected.
Deciding on when (and if) you need surgery for an injury is also sometimes not as easy as it sounds. Some injuries (e.g. knee or shoulder injuries) might initially seem terrible, but will recover well with good rehabilitation, and without surgery. Other injuries might not seem too bad, but will not do so well without an operation. It takes experience to help make these decisions, and our Acute Injury Clinic is designed specially to provide this service.
Can I get a scan today?
Not all injuries need further scans or tests, but if they do we can arrange to get them done right next door at Lake Imaging. Exactly what sort of scan is the best one is sometimes not as simple as you would think, which is why our specialist knowledge of injury management is important.
Who will you see?
At the Acute Injury Clinic you will see one of our sports doctors. Our senior Sports Physiotherapist will be there too if you need to see him too.
What do we do?
The Ballarat OSM Acute Injury Clinic is a unique model of care aimed at providing rapid, expert advice on treating new sporting and other injuries.
While hospital Emergency Departments are excellent at deciding if you need urgent treatment (e.g. surgery for very bad fractures), for most other injuries the treatment options can vary from rest, to rehabilitation, to surgery at some time later. The best course of action is often not easy to determine straight away. Getting the right advice about how to treat your injury is the most important first step in getting better.
When we see you within a few days of your injury, we can assess the severity of the injury, discuss the need for any further scans or tests, and start the decision making about the best way of treating YOUR injury.
We will also start you on a rehabilitation program, with early exercises and treatments to make your recovery as quick and as smooth as possible.
We can also arrange follow-up appointments with our Sport & Exercise Medicine Physician, with our (or your usual) physio, and with the most appropriate surgeons if that is the best course of action.
Bruising after Joint Replacement Surgery
Bruising after a Total Hip or Total Knee Replacement is normal. For some, the bruising can be mild, whilst for others the bruising can be extensive in nature.
After a Total Knee Replacement, some people may have bruising in the thigh, around the knee, down the shin, extending to the ankles and even toes.
In Total Hip Replacement, some people may have bruising around the suture line, into the buttock or groin. For some the bruising may extend down toward the knee, and for some even to the ankles/toes. Deep bruising may appear less intense and take longer to appear. A corked thigh sensation is something that is not uncommon after hip replacement. This is due to deep bruising in the thigh muscle.
What is normal?
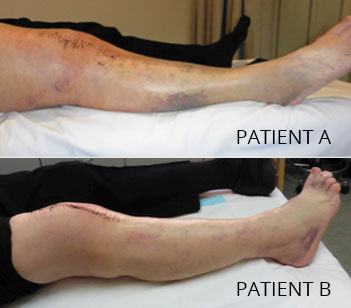
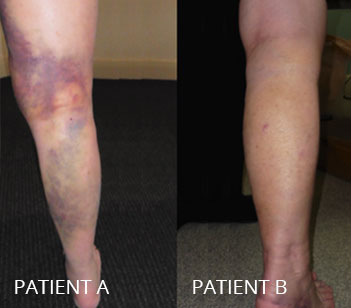
Below are photos of patients after Total Knee Replacement. Both are female, and not on any blooding thinning medications prior to surgery. The photos are taken at day 11 after surgery at the post-op appointment in the rooms. (The bruising may have been more severe a few days earlier)
{kind=link}
{kind=link}
Whilst extensive bruising may seem ‘alarming’, it is also short term and normal. Differences as to why some people bruise more than others are varied, but can include- blood thinning agents (aspirin, warfarin, xarelto), the nature of surgery itself, skin tones & colourings, and areas of loose skin. Additionally, some people have a propensity to bruise more easily.
Bruising usually begins to fade and disappear during week 2 after surgery.
Similarly you will notice the change in colour of the bruising- from deep red/purple, to greenish, to a yellowish type hue before fading completely.
What can be done to expedite healing of bruising?
In the initial post operative phase applying ice can be beneficial. Ice should not be applied directly to the skin. A bag of frozen peas, or ice packs, in a pillowslip is ideal. Elevation of limbs is also helpful. These both help with the degree of swelling, which can help with discomfort after surgery.
Remember bruising is short term and normal. However, please contact the rooms if you have any concerns.
Sleeping & Eating after Joint Replacement
After surgery, normal sleeping and eating patterns can be altered.
Why?
There are many theories as to what causes changes in sleep and appetite after surgery-
- the anaesthetic
- the surgery
- blood loss
- change in bowel habits
- fatique
- pain
- post operative medications
- change to normal routine after surgery.
In truth, it can be a combination of all or none of these theories.
Generally speaking, there is nothing to be alarmed about.
It is more important to eat small, regular, light meals. Ensure that you have adequate fluid intake. Avoid coffee or tea in the evenings. Take the prescribed painkillers if it is difficult to get comfortable. It is often better to take these medications prior to going to bed, rather than spending the night being uncomfortable and unsettled.
If people aren’t sleeping reasonably when we see them at 12 days after surgery, we often prescribe a tablet for nerve pain that also works as a mild sedative, getting the sleep/wake cycle back on track.
In time things should return to normal, but in the interim try not to dwell too much on these changes and focus on getting back to life.
Constipation after Joint Surgery
Constipation after joint replacement surgery can be a common occurrence. It is something we strive to avoid.
What actually is constipation?
There are many definitions of constipation. Constipation is the inability to pass faeces or having difficulty passing faeces, because it is dry or hardened. We all have our own “normal” pattern for bowel movements- for some that may be 2-3 times a day, for others 2-3 times a week. Alterations to this normal pattern can be classed as constipation to the individual. So if you use your bowels three times a week prior to surgery, then there is no reason for concern. However for those that use their bowels daily, a change to 2-3 times a week is classed as constipation.
As the time frame of constipation increases so to does its severity. As the length of time between bowel movements increases, more water is absorbed back into the bloodstream, causing the stool to harden in the colon. The discomfort increases, along with the damage that can be done by straining to have a bowel movement. As a result there can be symptoms of reduced frequency of bowel motions, difficulty and straining when passing bowel motions, passing small, hard, lumpy stools; and a feeling of incomplete/inability to empty the rectum. Additionally some people experience abdominal bloating, generalised feeling of being unwell and loss of appetite. Occasionally, some people complaining of diarrhoea may in fact have ‘overflow’ diarrhoea as a result of constipation.
What causes constipation after surgery
Post-operative patients are prone to constipation for a variety of reasons:
- Pain Medications prescribed
- Change in eating and drinking habits
- Change in activity levels
- The anaesthetic
- Change in daily routine-
- different bathroom/toilet
- sharing bathroom/room with others
- different surroundings
Preventing and Treating Constipation
If you are prone to constipation please mention this to your surgeon. A stool softener (Movicol) is often prescribed in hospital and you may also be discharged home with Movicol.
- Drink plenty of fluids- water and fruit juices.
- Eat plenty of fruit/vegetables
- Ensure that you get adequate walking/exercise.
Why is Constipation a Big Deal After Surgery?
Constipation can progress to impaction. Impaction is when the stool is so hard and dry that you cannot have a bowel movement. The hardened stool must be removed by enemas, manual disimpaction or (in advanced cases) surgery.
If your bowels have not worked within three days of surgery please seek advice from your local Pharmacy. If they still haven’t worked the next day – contact you surgeon. It is more advisable to act promptly rather than to wait until the situations escalates and hospitalisation is required.
Common Medications prescribed after Joint Replacement Surgery
What are they all for?
Cartia (aspirin)
Cartia reduces the stickiness of platelets (component of our blood) and stops the platelets clumping together to form blood clots. Cartia decreases the risk of heart attacks, strokes and Deep Vein Thrombosis (DVT) after surgery. Routinely used for 6 weeks after surgery.
Other anticoagulants might be used instead – including warfarin, plavix, clexane and xarelto. The type of anti-coagulant varies between patients and considers other factors (heart disease, previous stent surgery, AF, previous DVT)
Panadol (paracetamol)
Panadol is a painkiller. It can be used for mild pain, but we most commonly use it after surgery as background to enhance the effect of other medications – it is certainly useful in the first three weeks from surgery.
Mobic or Celebrex (anti-inflammatories)
These medicines work by reducing hormones that cause inflammation and pain in the body. It is used to relieve the symptoms of joint pain, tenderness, swelling and stiffness. They prevent a condition called heterotopic ossification, or unexpected bone formation, which once was commonly seen after hip replacement surgery. Typically we use these medications for three weeks after surgery.
Somac (pantoprazole)
Somac belongs to a group of medications known as proton pump inhibitors. It decreases the amount of acid produced by the stomach. In joint replacement surgery it is prescribed to prevent ulcers associated with the use of non-steroidal anti-inflammatories and aspirin. Somac can assist with nausea and reflux.
Movicol
Constipation and its sequel is our most common complication of surgery. Movicol is a type of laxative. It assists in keeps the bowels moving. It relieves constipation by increasing the water content and volume of the stools in the bowel, making them softer and easier to pass. Immobility, change in routine, anaesthetics and pain relieving medications can all increase the risk of constipation after surgery. Movicol, fluid, and walking is the solution.
Norspan Patch (buprenorphine)
Buprenorphine belongs to a group of medicines called opioid analgesics (like morphine). Norspan patches are used as a constant background for moderate to severe pain. The drug passes through the skin into the blood. We often have the patients change the patch six days after surgery, and then further instructions after we see you in the post operative clinic. Shorter cooler showers are better to avoid the patch releasing too much drug and making you dizzy. If you have no pain, it may cause nausea and need to be removed. Phone the ward or your surgeon for advice before removing.
Tramal (tramadol)
Tramal is a pain killer, either by itself, or in combination with other drugs – like the above list. Tramal works in a number of ways within the brain to reduce pain. In theory, it can interact with antidepressants, but most people on normal doses won’t have a problem. It works for 93% of our patients – but the others can experience hallucinations or nausea from it.
Endone
Endone belongs to a group of medicines called narcotic analgesics (like morphine, heroin and codeine). Narcotic analgesics act to “distance oneself” from pain. It is used to relieve moderate or severe pain after surgery. Some surgeons prefer endone instead of tramal.
Powerade
OK – this isn’t really a medication, but by having some clear fluid with a little salt and glucose in your stomach, it seems people wake up after surgery in better shape and with more energy. We ask that you drink at least half a bottle of Powerade one hour prior to your admission time at hospital. The anaesthetist will allow you to have clear fluids up until two hours prior to surgery.
Please inform your surgeon of any allergies and ensure your surgeon is aware of any medications you are taking.