FIFA Women's World Cup – It’s on our doorstep!
A summary on meniscal injuries by Professor Romain Seal consultant knee and cartilage surgeon to Aspetar Sports and Orthopedic center of excellence can be viewed here
The FIFA Women’s World Cup is just days away. There are 8 groups of 4 teams in the first round robin stage. Australia will play Canada, Ireland and Nigeria after which the top two teams in our group will progress through to the knockout round of 16 matches.
After the FIFA Men’s World Cup, this will be the most watched sporting tournament world- wide. And Australia is hosting!!
This blog is the fourth in a series brought to you throughout the tournament where Ballarat Sports Medicine and BallaratOSM will focus on injuries in soccer. In this blog, the focus moves to the knee for Meniscal Injuries.
Meniscal Injuries
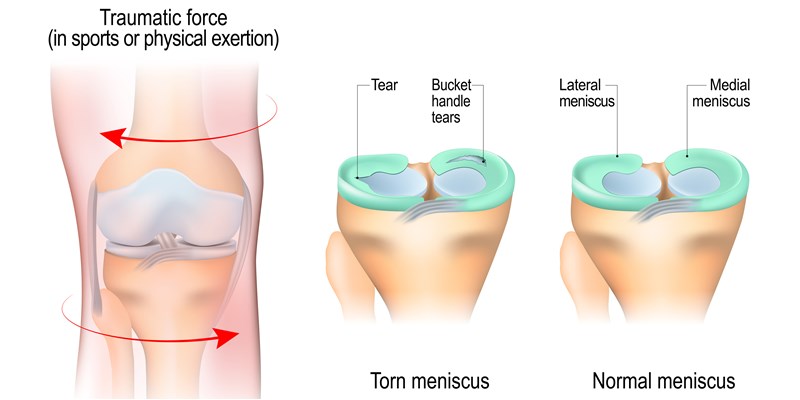
Meniscal injuries are among the most common knee injuries, and they come in different degrees of severity.
There are two different menisci in both knees. They lie on each side of the knee joint and function as shock absorbers and stabilisers. The meniscus on the inside is called the medial meniscus and the one on the outer part is called the lateral meniscus.
Twisting injuries
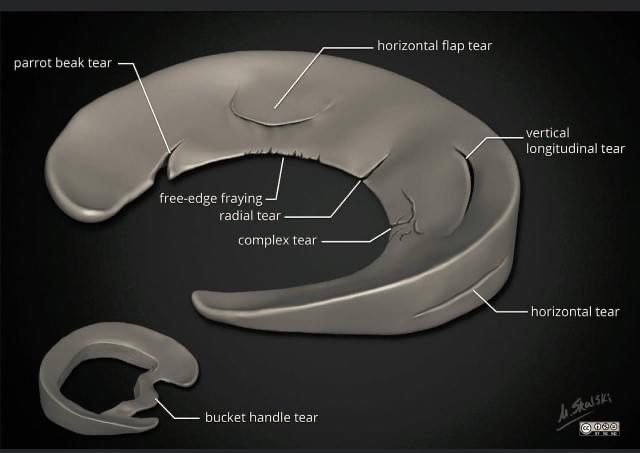
Meniscal injuries come in different forms which require different treatment approaches. Acute injuries occur when twisting the knee, and are most common in young athletes. Age-related changes or “injuries” in the menisci occur over time, affecting the middle-aged and the elderly. These age-related changes are a result of the body ageing on the inside, similar to what it does on the outside. Some hurt and some do not. Many knees have so called degenerative injuries (age-related changes), but no pain. We do not know exactly why that is.
Acute injuries often require surgery, either by removing part of the meniscus or by repairing it. The latter takes a long time to recover. Age-related changes are predominantly treated with a structured rehabilitation program and most recover without surgery.
Meniscal injuries can increase your risk of osteoarthritis. How big that risk is depends on the severity and location of the injury.
Injury mechanism, signs and symptoms
Most acute injuries are twisting injuries with the foot firmly placed on the ground. The degree of pain varies a lot. Some feel like something has been torn. Smaller injuries will not necessarily give immediate symptoms, but normally you will get pain and swelling within 24 hours after the injury occurred. With older athletes, a small tear in the meniscus can occur with minimal trauma.
Severe injuries normally give severe symptoms. Shortly after injury there is pain and decreased ability to bend and stretch the knee. It is also common the injured athlete can experience locking of the knee with or without clicking noises. This is also a common feature of anterior cruciate ligament (ACL) injury.
MRI imaging can help to determine the location and severity, but this is not always necessary.
Treating acute meniscus injuries
Treatment is dependent on the severity of the injury, size of tear, symptoms, and future requirements of the knee. On one end of the spectrum is a small tear, but without locking and limited range of motion. These might heal conservatively (without surgery) but sometimes follow-up shows they have not.
On the other end of the spectrum is severe and painful injuries, where the knee is locked in certain positions. These require immediate surgery with so-called arthroscopic surgery. This is keyhole surgery, using instruments that can be introduced through small (roughly 8-10mm) incisions. The decision to undergo surgery should be based on the severity of signs and symptoms, as well as the requirements for activity in the future.
Rehabilitation after surgery
Rehabilitation is affected by the severity of the injury. If a small piece of the meniscus has been removed, the athlete will be able to return to sport relatively quickly. Often within four weeks. More severe injuries with additional injuries to cartilage and ligaments will prolong the rehabilitation period. If the athlete returns to sport too early, it can have dire consequences. Recurrent swelling and persisting pain is often a result of this.
Rehabilitation should be done in conjunction with a skilled physiotherapist. The meniscus will gradually be able to withstand more weight-bearing activities. This should be incorporated in the rehabilitation program by gradually increasing physical requirements – if the knee can tolerate it.
Treatment of age-related injuries
Not so long ago, all meniscal injuries were treated the same – with surgery. Recent research, however, has shown that degenerative meniscal injuries should be treated with structured training. Exercises aim to strengthen the muscles around the knee, to increase body control and balance. It may take several months before the knee pain goes away, but results are as good as surgery.
Have a sore knee?
You can have your knee pain expertly diagnosed at Ballarat Sports Medicine. Sport & Exercise Medicine Physician, Dr Greg Harris and Sport & Exercise Medicine Registrar, Dr Jai Sharma can determine whether you may need surgery or not. If you do require surgery they may refer you to BallaratOSM’s independent surgeons, Mr Luke Spencer, Mr Shaun English, Mr David Mitchell, Mr Lawrence Tee, Mr Scott Mason or Mr Naveen Nara to assess the injury further with a view to provide surgical intervention to repair the damaged meniscus. Physiotherapists, Luke Blunden, Peta Johnston and Simon Lewis are all highly qualified to rehabilitate your knee.
References: https://fittoplay.org/sports/football/
