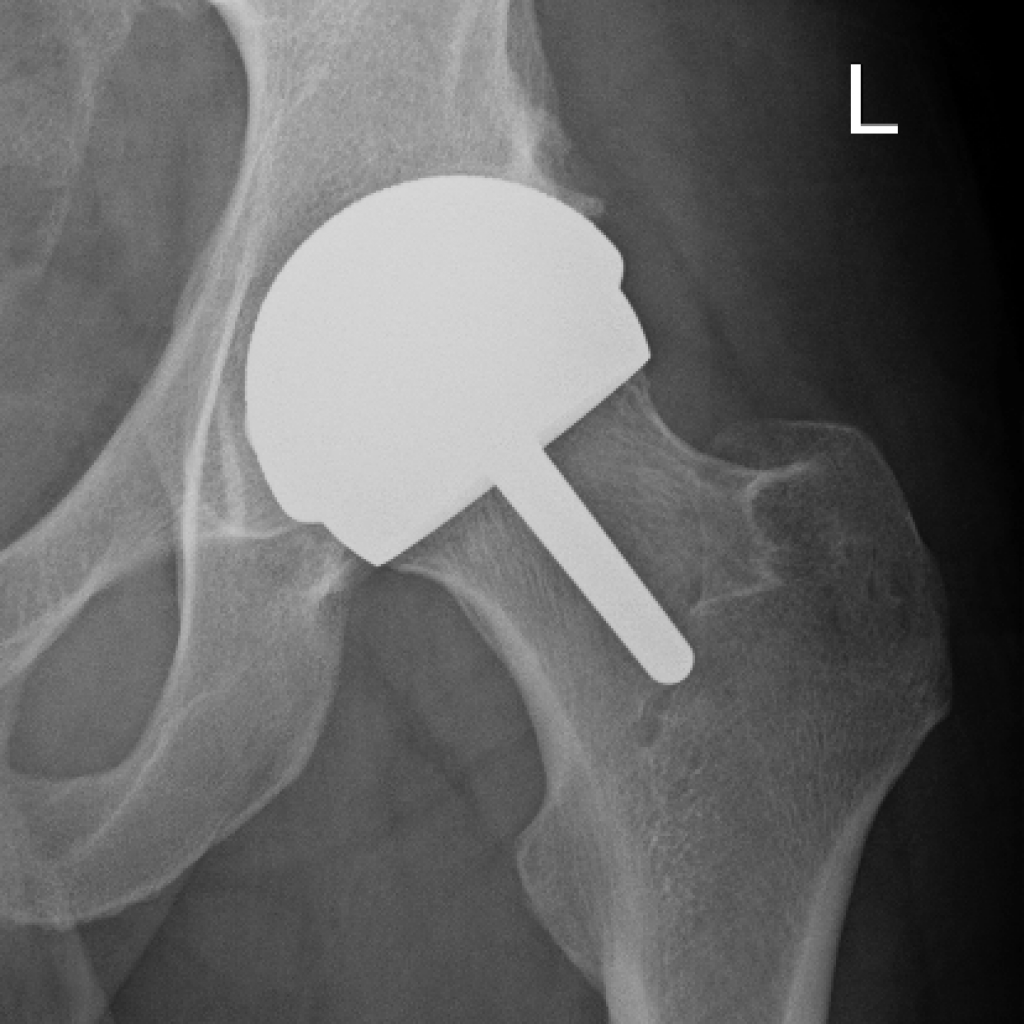
Hip

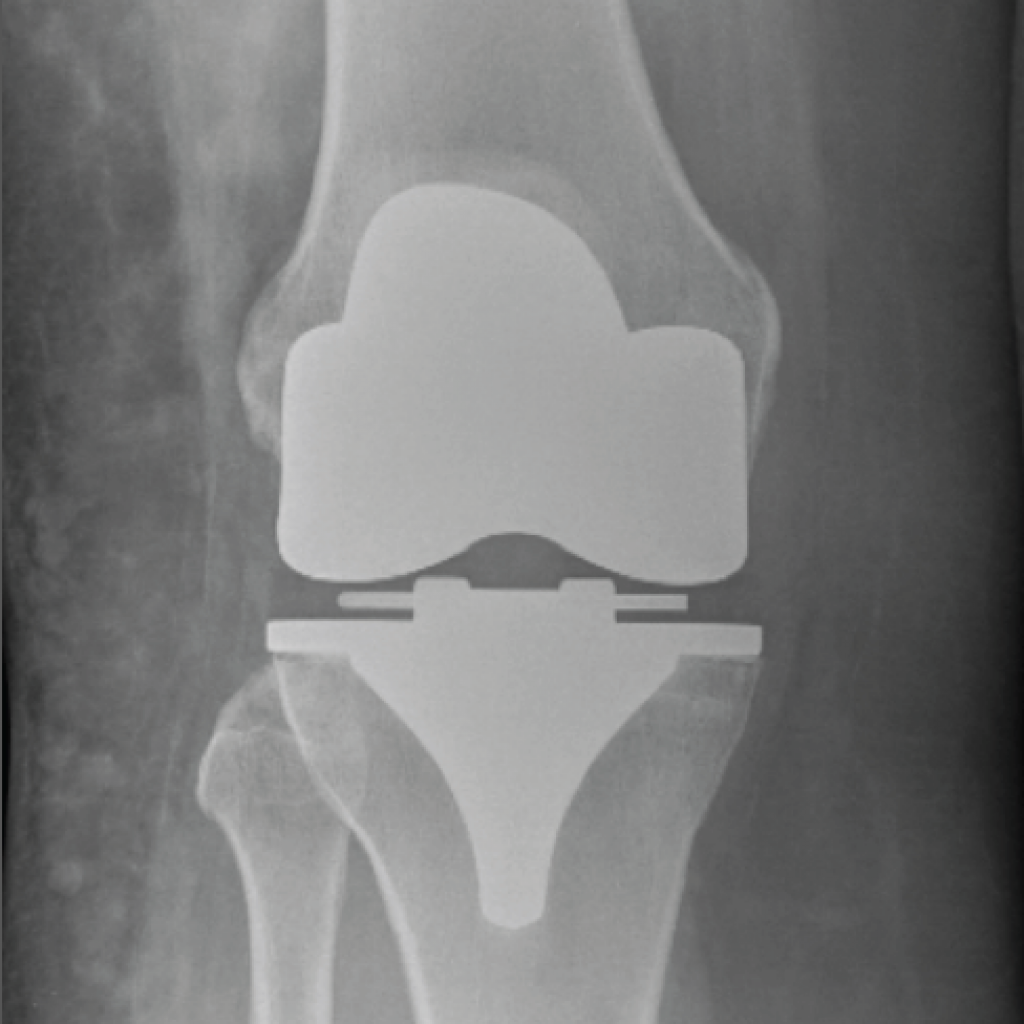
knee

Shoulder


Ankle




Elbow
- All
- Sports Medicine
- Orthopaedics
- Novar Specialists

Sports Medicine

Hands and Wrists

Knees

Rapid Recovery Surgery

Psychology

Shoulders & Arms

Physiotherapy

Medical Clearance Assessments

Joint Replacement

Foot & Ankle

Hips & Hamstrings

Trauma

Spine Surgery

LIPUS

Shockwave Therapy
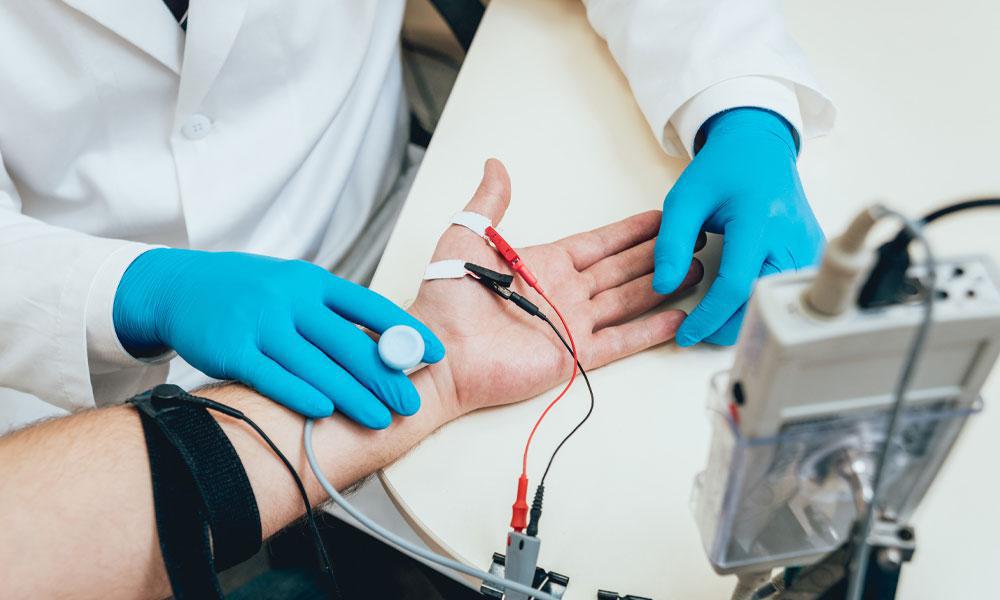
Neurology

Myotherapy

Exercise Physiology

Tendon Treatments

PRP Injections

Iontophoresis

Autologous Blood Injections (ABI)
